Introduction
Physical therapy in Elko for Upper Back Issues
Welcome to Pinion Rehabilitation's guide to Scoliosis.
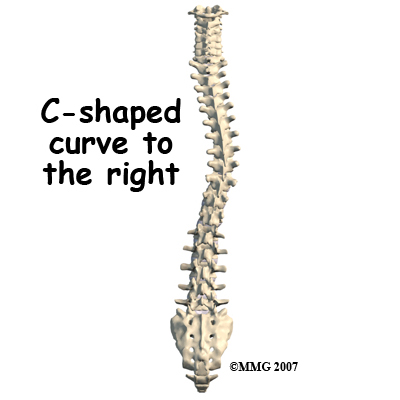
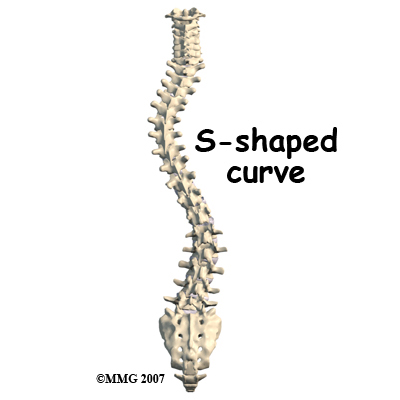
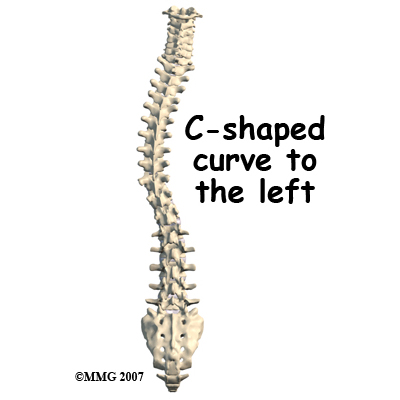
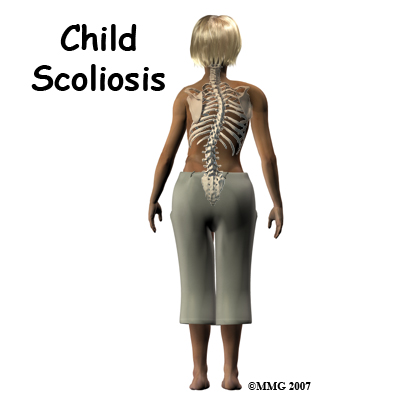 Scoliosis is a deformity in the spine that causes an abnormal C-shaped (one curve) or S-shaped (two curves) curvature. The spine is not straight but curves to one or both sides.
Scoliosis is a deformity in the spine that causes an abnormal C-shaped (one curve) or S-shaped (two curves) curvature. The spine is not straight but curves to one or both sides.
There are three types of scoliosis that are categorized based on when it develops. Infantile scoliosis occurs from birth to three years of age. Juvenile scoliosis develops between four and nine years of age. Adolescent scoliosis presents between 10 years and when growth is complete. Adults do not generally develop classic scoliosis but rather can have residuals of childhood scoliosis.
This guide will help you understand:
- what parts of the spine are involved
- what causes the condition
- what treatment options are available
- what Pinion Rehabilitation’s approach to rehabilitation is
Anatomy
What parts of the spine are involved?
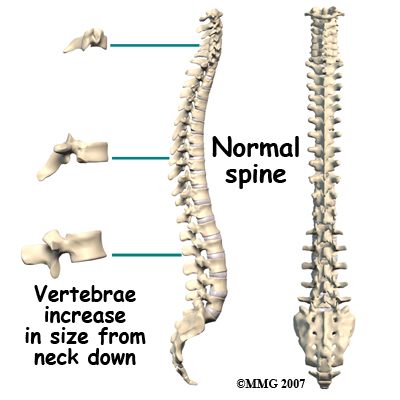
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The spinal column is the body's main upright support.
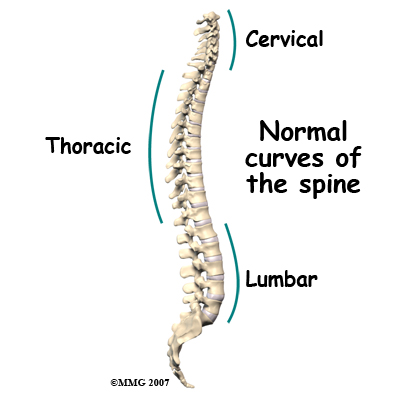
When viewed from the side, the spine forms three curves: The neck, (called the cervical spine) curves slightly inward, the thoracic spine curves outward, and the low back (called the lumbar spine,) like the cervical spine, also curves inward. When viewed from the back, the vertebrae form a straight column keeping the head centered over the body.
Each vertebra is made of the same parts. A round block of bone, called the vertebral body, forms the main section of each vertebra. Each vertebra increases slightly in size from the neck down. The increased size helps balance and support the larger muscles that connect to the lower parts of the spine. Each section of vertebrae, however, the cervical, thoracic, and lumbar, are anatomically a bit different from each other in order to accommodate each area’s particular function for the body.
Causes
How does scoliosis develop?
 Sometimes it is not known why a scoliosis develops. If the specific cause is unknown, it is termed idiopathic. Idiopathic scoliosis is the most common type of scoliosis and affects about two to three per cent of the population. It tends to run in families and is more common in girls than in boys. Most often the scoliosis develops in middle or late childhood during a rapid growth spurt.
Sometimes it is not known why a scoliosis develops. If the specific cause is unknown, it is termed idiopathic. Idiopathic scoliosis is the most common type of scoliosis and affects about two to three per cent of the population. It tends to run in families and is more common in girls than in boys. Most often the scoliosis develops in middle or late childhood during a rapid growth spurt.
Scoliosis can also be congenital (present at birth) or it may develop as a result of another neurological condition such as cerebral palsy, spina bifida, or spinal muscular atrophy.
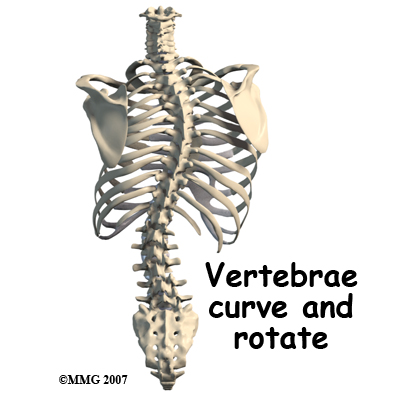
Any part of the spine can be affected by scoliosis, however, most often the thoracic and then lumbar spines are affected. The vertebrae curve to one side and may rotate, which makes the waist, hips, or shoulders appear uneven. At first, a C-shaped curve may develop causing the shoulders and hips to tilt down on one side. In an effort to keep the head in the middle, the spine may compensate by curving the lower part of the spine in the other direction, forming an S-curve.
The most common curve in infantile idiopathic scoliosis is in the low thoracic region. Single curves are almost always in the thoracic region with variable amounts of vertebral rotation. As the vertebrae rotate, the attached ribs shift causing a noticeable rib bump or hump, as it is called, on one side of the spine. This hump is most obvious when the child is bent forward at the waist.
Most scoliotic curves (85 per cent) are to the right when they occur after the age of two years. A major thoracic curve forming before the age of five is most likely to result in other complications. Infantile idiopathic scoliosis with the thoracic curve to the left occurs most often in boys observed before one year of age. This type of scoliosis tends to resolve on its own without treatment and it does not get worse with puberty or during growth spurts.
Juvenile idiopathic scoliosis develops in boys at an earlier age than in girls. As boys mature skeletally at a later age than girls, this means there is a greater risk of curve progression in boys with this type of scoliosis compared to girls. The typical curve patterns of juvenile and adolescent idiopathic scoliosis are similar with right thoracic and double major curves present most often.
Symptoms
What does this condition feel like?
Scoliosis as it occurs is a painless condition. Someone with scoliosis may not feel any change in the spine but instead notice that their clothes don't fit quite right or that their posture is not straight. In children, the parent or a teacher often notices an asymmetry. As the spine starts to curve, the body adjusts to keep the head in the middle over the pelvis.
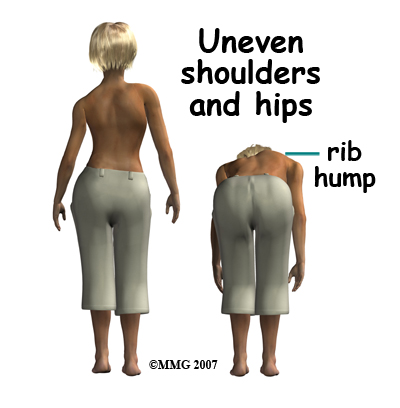 As a result, the shoulders and hips may be uneven, causing one shirtsleeve or pant leg to seem shorter than the other. Often there is rotation of the vertebrae causing an uneven waist so that a pair of pants or skirt twists to one side.
As a result, the shoulders and hips may be uneven, causing one shirtsleeve or pant leg to seem shorter than the other. Often there is rotation of the vertebrae causing an uneven waist so that a pair of pants or skirt twists to one side.
The most common noticed signs of scoliosis are:
- uneven shoulders
- uneven hips
- uneven breasts (girls) or nipples (boys and young girls)
- prominent or winging shoulder blades particularly on one side
- leaning to one side
- bump or rib hump on one side of the spine, most noticeable when bending forward at the waist
The presence of one or more of these signs suggests a need for a medical exam by a pediatrician, primary care physician, physical therapist, or orthopedic surgeon. Severe scoliosis can cause pressure on the heart, lungs, liver, and other internal organs. Early diagnosis and treatment are important to prevent problems with breathing and cardiovascular function.
While it is said that scoliosis itself is not painful, the curvature and resulting rotation of the spine can result in pain coming from the associated muscles, joints or ligaments as uneven pressure or tension is placed upon these structures.
Diagnosis
How do health care professionals identify the problem?
Many children are first identified as having scoliosis during a school-screening program by the school nurse or physical therapist. As mentioned above, a forward bend test (called the Adams test) is used to look for prominence of the ribs or changes in the spine, which indicate a scoliosis. During the Adams test the patient slowly bends forward at the waist as if diving into a pool while the health care practitioner observes the spine from behind the patient. Anyone with signs of scoliosis identified as a result of a school screening is referred to his or her family doctor who will examine the spine and look for the possible causes of scoliosis. X-rays are not ordered for every patient as they are often not required to diagnose a scoliosis. Not doing x-rays avoids needless exposure of growing children to radiation. However, if there are significant signs of asymmetry (unevenness) and other changes observed during the physical exam, an x-ray may be taken in order to radiologically view any tilt or rotation of the vertebrae. An MRI may be ordered if the physician suspects an infection, tumor, or problems in the nervous system that is causing the scoliosis.
When an x-ray is warranted to look at the curvature, the doctor will use a technique called the Cobb method to measure the location and degree of each curve. Curves must be more than 10-degrees to be considered a scoliosis.
X-rays may be taken also in order to identify skeletal maturation or bone growth. The Risser sign is applied to the x-rays of the pelvic bones to judge whether or not the child has stopped growing. The amount of spinal curvature is compared with the stage of growth activity to help guide treatment.
Treatment
What treatment options are available?
There are a few ways to treat scoliosis in children. These methods include doing nothing (only observing), using a brace, implementing exercises, or doing surgery. Treatment, usually in the form of exercises, can also be done for adults, but all treatment is most effective if started as early as possible and certainly before the child stops growing. That being said, studies show that 90 per cent of infantile scoliosis resolves or goes away on its own. In other words, the child will "grow out of it."
Selecting treatment options for the child with scoliosis involves several factors; the age of the child, the degree of the spinal curve, the skeletal maturity of the spine, and the preferences of the patient and family.
Choosing the optimal treatment largely depends on the degree or severity of the scoliosis. Physical examinations and x-rays taken over a period of time will help show if the scoliosis is staying the same or progressing. Curves 45 degrees or less are more likely to be treated conservatively with exercises or bracing. Curves that are changing rapidly or that are greater than 45 degrees may require surgery.
Nonsurgical Treatment
Treatment may be nothing more than regular observation especially if the curve is 30-degrees or less in a child who is no longer growing. If the curve is progressing and the child is growing rapidly, or if the curve is 30-degrees or more, the child is referred to a physical therapist for exercises and to an orthopedic surgeon for bracing and to monitor progression in regards to the potential need for a surgical option.
 The best bracing results occur in children with slowly progressing curvatures that are detected and treated early. Most braces are worn over a tightly fitting cotton T-shirt but under the clothes. While wearing the brace, physical activity is restricted.
The best bracing results occur in children with slowly progressing curvatures that are detected and treated early. Most braces are worn over a tightly fitting cotton T-shirt but under the clothes. While wearing the brace, physical activity is restricted.
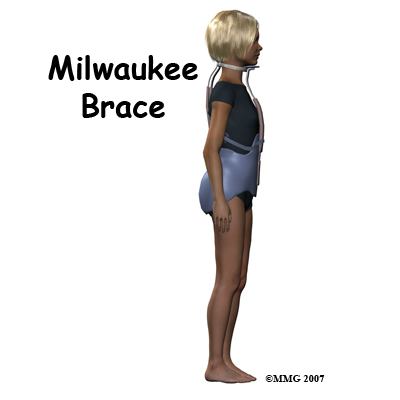
The two braces (orthosis) that are used most often for scoliosis are the Milwaukee brace and the Boston brace. The Boston brace is also called a thoracolumbosacral-orthosis or TLSO. Studies show that bracing for scoliosis controls the curve and prevents progression. In most cases, bracing does not correct the curve; it just keeps it from getting worse. Bracing is less likely to stop curves larger than 40-degrees and is more effective for single curves in the thoracic spine than for double curves.
The Milwaukee Brace is a corrective brace used with children and adolescents who have scoliosis. It has a pelvic girdle, two posterior uprights, one anterior upright, and a ring around the base of the skull that also supports the lower jaw. Originally made of leather and metal, it has been revised now and is constructed out of rigid plastic with metal uprights. Pads with straps attached to the frame are used to apply corrective forces.
The Boston Brace used for the treatment of scoliosis is very similar to the Milwaukee orthosis. The Boston brace does not extend up as high into the thoracic spine and it does not have the vertical bar in front of the chest or the cervical ring. The Boston brace works best for children who have immature spines or moderate scoliotic curves in the lower thoracic and upper lumbar spines.
While in the brace, your child won't be able to participate in sports that require flexibility such as gymnastics or tumbling. Physical contact sports such as football, hockey, or soccer are also prohibited while wearing the brace. Some children, with their physician's approval, are allowed to remove the brace for two to three hours each day and participate in sports during that time, but generally the brace is worn at all times.
Bracing is usually used for at least two years or until there is no sign on x-ray of further change. Your surgeon will follow your child at regular intervals. Follow-up visits and repeated x-rays are needed more often for the child who has a rapidly progressing curve or one who is in a growth spurt.
For many years, exercise was not considered effective in stopping or changing spinal curvatures from scoliosis. Recently, however, researchers have taken a closer look at exercise as a form of treatment. It has been found that in previous studies that discounted exercise, most of the children didn't do the exercises! Or, if they did, they only did them occasionally. Unless the exercise program was designed to prepare for a sports activity, compliance was very low.
Improved technology and the ability to assess muscle function have changed the picture in regards to the benefits of exercise for scoliosis. We now know that there is asymmetry in muscle function for everyone with scoliosis. More specifically, there is an uneven strength in trunk rotation. This asymmetry affects one’s posture, affects one’s appearance, can cause pain, and in more severe cases can affect the ability of one’s lungs to function to their full capacity since they are located in the area of the curved thoracic spine.
One of our physical therapists at Pinion Rehabilitation can guide your child through the appropriate exercise program to halt or slow progression of their scoliotic curve, decrease any associated pain, maintain or improve posture and appearance, as well as maintain the ability of the lungs to function well. Although recent studies mainly support progressive resistive exercises as being most effective for curves less than 45 degrees, all patients with scoliosis can potentially benefit from doing exercises that strengthen and stretch the muscles that have been affected, which can, in turn, can halt or slow the progression of the curve.
At your first visit to Pinion Rehabilitation your physical therapist will ask a number of questions regarding your child’s scoliosis, including when it was first noticed, if any x-rays or other investigative tests have been done, if there is any associated pain, what activities, if any, are limited due to the scoliosis, and they will also inquire about what current sports or activities your child partakes in (if they are old enough to do so.) They will also want to know whether or not a brace has been recommended or an orthopaedic surgeon has been consulted.
At the initial assessment your physical therapist will observe and palpate (feel) your child’s spine in standing, sitting, and in a face-down position, and will ask your child to perform a number of motions to assess the movement of the spine, such as side bending, leaning backwards and forwards, and twisting. They will look for a thoracic rib hump. As mentioned previously, when bending forward, due to the rotation of the vertebrae and the attached ribs, the ribs on one side create a ‘rib hump’, which is more pronounced the greater the curve.
Your physical therapist will also observe how your child’s shoulders, neck, hips, and low back move, as all of these areas can be adversely affected by a scoliotic spine, and will require specific exercises to maintain or regain their motion and strength.
Your physical therapist will also take some measurements of how well your child is moving. These measurements may be as simple as measuring how far your child can reach when they bend forward or twist.
Next your physical therapist will look for any abnormal tightness or elongation in the muscles around your child’s back, abdominal area, shoulders, hips, legs, and neck. In addition, they will also assess the degree of muscle imbalance present in your child around these areas, particularly the muscles of the back. With scoliosis the muscles of the back become tight and overly strong on the concave part of the curve or curves, and weak and elongated on the convex side.
Your physical therapist may also have your child perform some functional tests, such as lifting an item overhead, or jumping on one foot to determine how the scoliosis is affecting their ability to do everyday activities.
The next part of your child’s treatment at Pinion Rehabilitation will involve your therapist designing a specific exercise program that they will ask your child to perform both in the clinic as well as at home. Depending on the age of your child, your assistance may be required for the exercises. The exercises included will address each child’s specific needs, however, most scoliosis programs will include stretching exercises for the back, shoulders, hips and back of the legs. Also included will be strengthening exercises that involve rotation of the spine, extension of the spine and shoulders, side bending of the spine, and core stability exercises including tilting of the pelvis. Exercises for the hips will include focusing on strengthening the buttocks area as the buttocks plays a large role in supporting the low back, which in turn supports the thoracic spine. The use of exercise bands, weights, and weight machines will be incorporated once the technique of the exercises has been mastered. Using resistance with exercises has been proven, in some types of scoliosis curves, to be the key to halting the progression (or sometimes even reversing it mildly.) Some exercises may involve simply activating or tightening a muscle without actually moving the joint or limb (termed isometric exercises). Even though they do not involve motion, these types of exercises can assist in strengthening the required muscles to maintain good posture, and halt the progression of the scoliosis.
The advice of a physical therapist is crucial in regards to exercise technique, advancing exercises, or increasing the weight used with any exercise that is used to treat a scoliosis. Doing incorrect exercises or using too much weight could make a scoliosis worse or cause compensatory pain. As the scoliotic curvature causes an imbalance in the strength and length of the muscles of the body, don’t be surprised if your physical therapist at Pinion Rehabilitation asks you to do more repetitions or use heavier weights when doing an exercise on one side versus the other in order to start shifting the imbalance back towards a more neutral position.
As mentioned above, the curving and twisting of the spine has the potential to affect your child’s lung capacity as the lungs are located directly in front of the thoracic spine. For this reason it is important that your child performs deep breathing exercises or partakes in cardiovascular activities that encourage them to deep breath to maintain the lung’s capacity. Maintaining good posturing will also assist in maintaining lung function, therefore the final component to our treatment at Pinion Rehabilitation will be to provide education on maintaining good posturing as often as possible. As gravity is constantly pulling the body downwards, holding one’s body properly when walking, sitting, standing and during regular activities of daily living can make an enormous difference to how the muscles pull on the spine. Maintaining good posturing as often as possible is just as important in your child’s rehabilitation program as doing the specific exercises that your therapist prescribes.
Often exercises are used in conjunction with bracing when treating scoliosis. Unfortunately, there are cases where neither the bracing nor the exercises will assist in halting or slowing the progression of the scoliosis. In these cases, surgery may be required.
Pinion Rehabilitation provides services for physical therapy in Elko.
Surgery
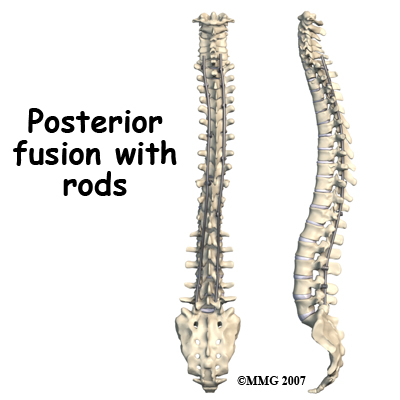 When surgery is performed for scoliosis metal rods or screws are used to help straighten and hold the spine in a corrected position. The vertebra are fused (joined together) to help correct the curvature. Luckily, only a small number of people with scoliosis require surgical intervention. New surgical techniques are designed to give maximum correction with a minimum of incisions and scarring.
When surgery is performed for scoliosis metal rods or screws are used to help straighten and hold the spine in a corrected position. The vertebra are fused (joined together) to help correct the curvature. Luckily, only a small number of people with scoliosis require surgical intervention. New surgical techniques are designed to give maximum correction with a minimum of incisions and scarring.
Surgery for idiopathic scoliosis is generally suggested when the curve is 50 degrees or more and bracing fails. Surgery is recommended with two goals in mind; 1) prevent progression of the spine deformity, and 2) to lessen the existing spine deformity. The surgical procedure most often used to correct idiopathic adolescent scoliosis is a posterior (through the back) fusion with instrumentation (rods, hooks, screws and wires) and bone grafting. Sometimes if the curve is severe, additional surgery may be required through the front of the body.
Scoliosis surgery is one of the most complicated orthopedic surgical procedures performed on children; the operation takes several hours.
Post Surgical Rehabilitation
Post-operatively, patients are usually discharged from the hospital within five to seven days.
Physical therapy at Pinion Rehabilitation can begin as soon as your surgeon allows. Generally children are able to progress quickly after surgery so that they can return to routine daily activities, including returning to school. The surgeon will set out any specific activity restrictions for your child.
The focus of our treatment at Pinion Rehabilitation after surgery for scoliosis will be to decrease any pain that remains from the surgical procedure itself, and to prescribe exercises that regain and maintain the mobility and strength of the back, shoulders, neck and hips. Core stability exercises will be of particular importance as these exercises ensure that the body has a strong central system to work from. We will also assist your child in learning to maintain a new normal posture as a result of the new position of their spine.
At the first few appointments post-surgically your child’s physical therapist may use modalities such as ice and heat to assist with your child’s pain. In some cases, and depending on where your child’s pain is, electrical modalities such as ultrasound or interferential current may also be used. Massage to the muscles or other hands-on techniques such as gentle traction to the joints may also be part of your child’s initial physical therapy treatment.
Next your child’s therapist will prescribe a series of stretching and strengthening exercises that focus on the core area, the back muscles, the shoulders, the hips, buttocks, back of the legs, and the neck. These exercises are designed to keep the muscles strong and flexible so that they reduce the pressure and pull on the spine and inserted rod. Extension and rotation exercises will be included in your child’s program as these types of exercises are particularly useful when treating the effects of scoliosis. As able, resistance in the form of exercise bands, free weights, or weight machines may be used. Due to the muscles imbalance that would have been present prior to the surgery, some muscles will be stronger or tighter than others, so again, do not be surprised if your therapist prescribes more exercises for one side than the other to combat this imbalance.
As discussed under non-surgical treatment, maintaining or increasing your child’s lung capacity will be crucial now that the scoliotic curve has been corrected. Deep breathing exercises along with cardiovascular exercises will be prescribed.
The final component to our treatment after surgery to correct a scoliotic curve will be education regarding maintaining proper posturing. It is often difficult for children to understand the importance of posture at such a young age, so frequent reminders by you, as the parent, will be important. Maintaining upright posturing as often as possible during all activities of daily living will assist in decreasing any stress put on the surgical rod as well as the muscles as they work to support the new position of the spine. Your physical therapist at Pinion Rehabilitation will demonstrate the optimal posturing that your child should work to achieve.
Generally the rehabilitation after spinal surgery to correct a scoliosis responds very well to the physical therapy we provide at Pinion Rehabilitation. If for some reason, however, your child’s pain continues longer than it should or their therapy is not progressing as your physical therapist would expect, we will ask you to follow-up with your child’s surgeon to confirm that the spine is tolerating the rehabilitation well and to ensure that there are no complications that may be impeding your child’s recovery.
Portions of this document copyright MMG, LLC.
Pinion Rehabilitation provides services for physical therapy in Elko.